

Exercise Prescription for Providers: Making Movement Meaningful, Measurable, and Actually Doable

Illustration of two healthcare providers working with a female patient in a bright clinic setting. One provider is holding a clipboard while the other gestures during exercise instruction, and the patient is kneeling on an exercise mat. The image includes the title “Exercise Prescription for Providers: Making Movement Meaningful, Measurable, and Actually Doable,” emphasizing collaborative, inclusive, and patient-centered exercise prescription.
Exercise prescription is not just “telling someone to work out.”
For healthcare providers, it is the clinical process of matching the right type, dose, intensity, progression, and support to a person’s current capacity, goals, health status, confidence, and life context.
The big takeaway?
The best exercise program is not always the most technically perfect one. It is the one the patient understands, performs safely, and can continue consistently.
For resistance training, common evidence-based targets include:
Strength: heavier loads, commonly ≥ 85% of 1-repetition maximum, for lower repetitions
Power: moderate-to-heavy loads moved with intent and speed, depending on single-effort or repeated-effort goals
Hypertrophy: moderate-to-heavy loads, commonly 6–12 repetitions, with enough weekly volume
Muscular endurance: lighter loads, higher repetitions, and shorter rest periods
But exercise prescription should not stop at physiology.
It also needs to include education, shared decision-making, progression, confidence-building, and follow-up. Exercise works through the body, but adherence works through the relationship.
That is where providers matter.
🧾 General Information
Exercise Is Medicine — But Prescription Still Matters
Most clinicians agree that exercise is good for people.
That part is not controversial.
Exercise can support cardiovascular health, metabolic health, musculoskeletal function, mental health, pain management, healthy aging, and quality of life. But the clinical question is not simply:
“Should this person exercise?”
The better question is:
“What kind of exercise, at what dose, for what goal, with what support, and with what progression?”
That is exercise prescription.
A strong prescription considers the classic FITT framework:
Frequency: How often?
Intensity: How hard?
Time: How long?
Type: What kind of exercise?
For providers, the next step is making FITT more human.
Because patients do not live inside clinical guidelines. They live inside busy schedules, pain experiences, fear, fatigue, prior failures, insurance limits, family responsibilities, and real-world barriers.
So, while the science helps us dose movement, the relationship helps us deliver it.
Mechanotherapy: Why Loading Tissue Matters
One of the most useful concepts for providers is mechanotherapy.
Mechanotherapy describes how appropriately applied mechanical loading can stimulate tissue repair, remodeling, and adaptation. Khan and Scott describe this process through mechanotransduction, where cells sense mechanical load and respond biologically.
In plain language: The body listens to load.
When we apply the right amount of stress through movement, the body can respond by getting stronger, more tolerant, and more capable.
This is clinically relevant for many musculoskeletal concerns, including:
Tendinopathy
Muscle injury
Osteoarthritis
Bone health
Post-operative recovery
Deconditioning
Chronic pain-related activity avoidance
But the word “right” matters.
Too little load may fail to create adaptation.
Too much load may flare symptoms, reduce confidence, or exceed tissue capacity.
A well-designed exercise prescription helps patients move from:
“I hope this does not hurt me”
to
“I understand why I am doing this, how to do it, and how we will progress it.”
That shift is powerful.
Resistance Training: Matching the Goal to the Dose
Resistance training can be used to improve strength, power, hypertrophy, muscular endurance, function, confidence, and long-term health.
However, different goals require different programming decisions.
A general framework from strength and conditioning principles includes the following:
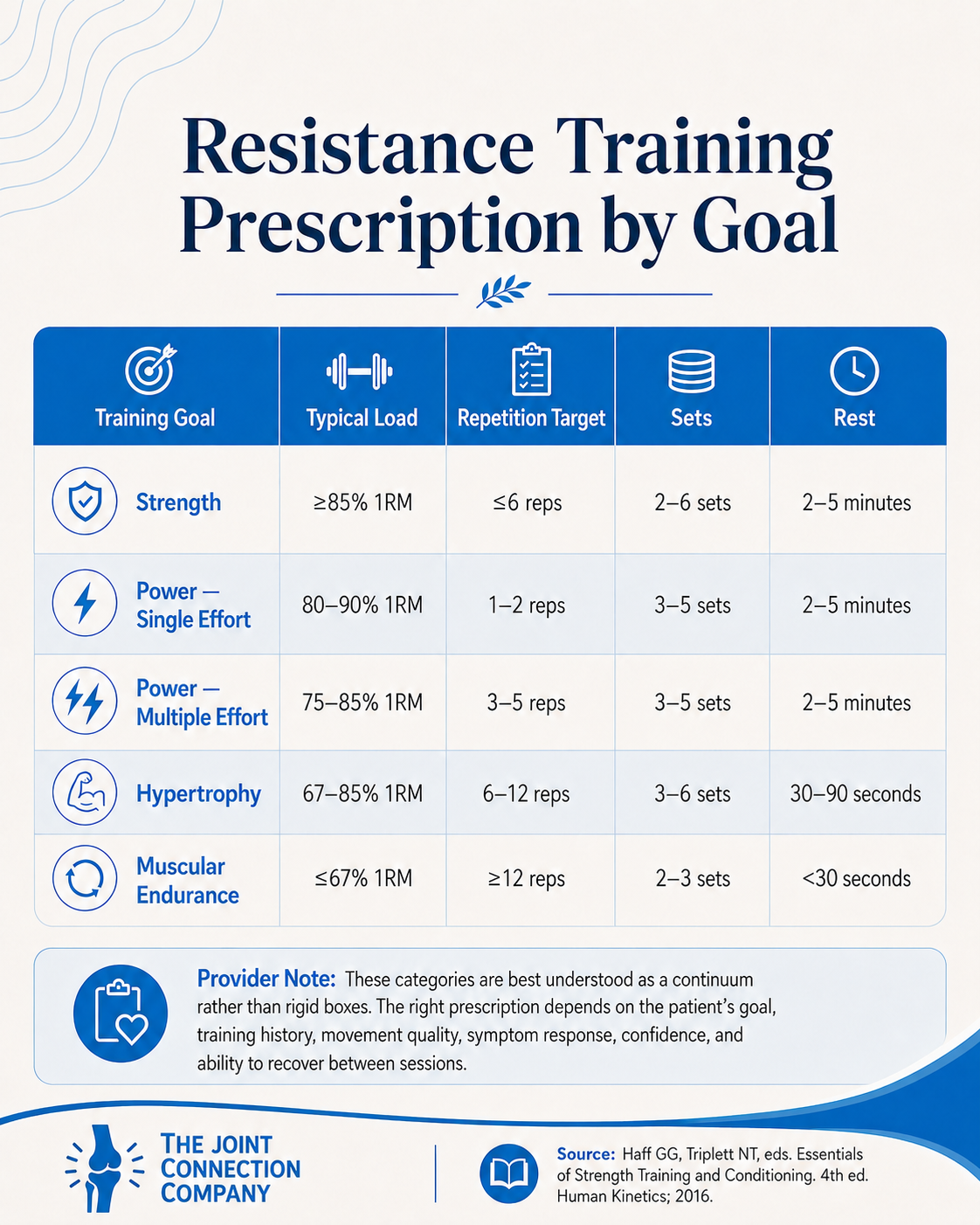
These categories are helpful, but they should not be treated as rigid boxes.
They exist on a continuum.
A patient doing 10 repetitions is not magically “hypertrophy only.” A patient doing 15 repetitions is not suddenly in a completely separate universe. Load, effort, volume, tempo, symptoms, rest, exercise selection, and training history all matter.
The better clinical question is:
“What adaptation are we trying to create, and what dose is realistic for this patient today?”
Start With Training Status, Not Just the Diagnosis
Two patients can have the same diagnosis and need completely different exercise prescriptions.
Why?
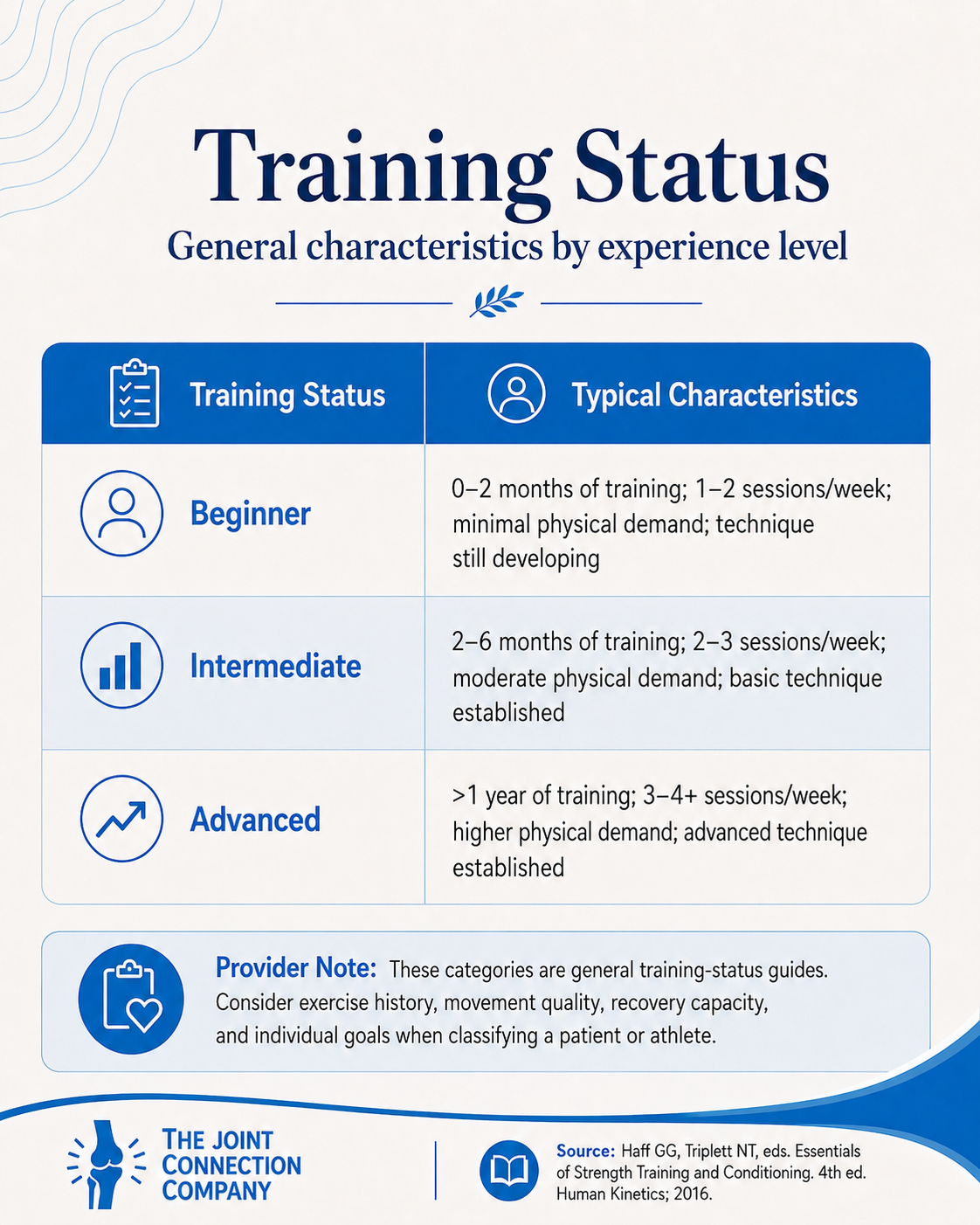
Because training status changes everything.
A beginner, intermediate, and advanced exerciser may respond differently to the same exercise, the same load, and the same volume.
A simple classification model includes:
This matters because “appropriate intensity” is not just about percentages.
It is also about:
Movement competency
Confidence
Symptom irritability
Medical history
Fear of movement
Recovery capacity
Access to equipment
Patient goals
Familiarity with resistance training
For example, a heavy deadlift variation may be a reasonable strength intervention for one patient and a completely inappropriate starting point for another.
Same movement category.
Different clinical decision.
Technique Before Intensity
Before loading someone heavily, providers should assess whether the patient can perform the movement with adequate control, coordination, and tolerance.
This does not mean every repetition needs to look like a textbook.
But it does mean the person should be able to perform the exercise safely enough for the intended goal.
When higher loads are introduced, especially for strength and power development, form and control become increasingly important.
Providers can adjust difficulty by changing:
Load
Range of motion
Tempo
Speed
Base of support
Surface stability
Direction of movement
Eyes open versus eyes closed
Single-task versus dual-task demands
Bilateral versus unilateral loading
Machine, cable, free weight, band, or bodyweight setup
This is one of the most underappreciated parts of exercise prescription.
Progression does not always mean “add more weight.”
Sometimes progression means:
Same weight, better control.
Same movement, more range.
Same exercise, slower tempo.
Same task, more confidence.
Same goal, fewer symptoms afterward.
That counts.
Heavier Loads Help Strength — But Adherence Still Wins
The 2026 American College of Sports Medicine overview on resistance training prescription supports several clinically useful points:
Resistance training is effective for improving strength, hypertrophy, physical performance, and health-related outcomes.
Training at least 2 days per week is a practical minimum for many adults.
Heavier loads are generally more effective for maximizing strength.
Hypertrophy can occur across a wider range of loads, especially when volume and effort are sufficient.
Many variables that clinicians debate — such as equipment type, timing, and complex programming details — may be less important than consistency and appropriate progression.
This is clinically freeing.
It does not mean details never matter.
It means providers should avoid letting perfect programming become the enemy of participation.
For many patients, the biggest barrier is not whether they should rest 90 seconds or 2 minutes.
The bigger barriers are:
“I do not know what to do.”
“I am afraid I will make it worse.”
“I do not have time.”
“I tried before and failed.”
“I do not feel strong enough to start.”
“I do not know what pain is acceptable.”
“I need someone to help me make sense of this.”
That is where healthcare providers can make the difference.
Exercise Prescription Is Also Behavior Change
A technically excellent exercise program that a patient never performs is not clinically effective.
Lucini and Pagani make an important point: an exercise prescription may be considered correct only if the person actually performs the exercise and the exercise produces the intended physiological or functional benefit.
That should stop us in our tracks.
Because it means exercise prescription is not only a technical skill.
It is also a communication skill.
Providers need to consider:
Does the patient understand why this matters?
Does the patient believe this is safe?
Does the patient feel capable?
Does the plan fit their life?
Does the patient know what to do if symptoms change?
Is there a follow-up plan?
Is the goal meaningful to the patient?
This is where motivational interviewing, shared decision-making, realistic goal setting, and patient education become essential.
A simple provider script might sound like:
“Based on what you told me, our goal is not just to make this muscle stronger. Our goal is to help you trust your body again when you lift, walk, climb stairs, or get back to the activities you care about. We will start with a dose your body can handle, then progress it together.”
That is exercise prescription with connection.
👩⚕️ For Providers 👨⚕️
1. Prescribe for the Goal, Not the Exercise Name
“Squats” are not a goal.
“Rows” are not a goal.
“Bridges” are not a goal.
They are tools.
Before choosing the exercise, identify the target adaptation.
Ask:
Are we trying to improve maximum force production?
Are we trying to improve repeated effort tolerance?
Are we trying to build muscle mass?
Are we trying to improve confidence with a functional task?
Are we trying to increase tissue capacity?
Are we trying to improve balance, power, coordination, or endurance?
Are we trying to reduce fear and restore participation?
The same exercise can be prescribed differently depending on the goal.
For example, a sit-to-stand can be:
A strength exercise if loaded heavily for fewer repetitions
An endurance exercise if performed for higher repetitions
A power exercise if performed quickly with safe intent
A balance exercise if altered with stance or surface changes
A functional confidence exercise if tied to daily activities
This is where providers move beyond “exercise sheets” and into clinical reasoning.
2. Use 1RM Carefully — and Consider Alternatives
One-repetition maximum testing can help estimate appropriate loading, especially for strength-focused programming.
However, true 1RM testing is not always necessary or appropriate.
In many clinical populations, providers may use:
Estimated 1RM
Multiple-repetition maximum testing, such as 5RM
Rate of perceived exertion
Repetitions in reserve
Symptom response
Functional testing
Submaximal loading
Movement-quality assessment
The key is not always finding the perfect number.
The key is finding a safe and useful way to answer:
“How hard is this for this person?”
For higher-risk patients, medically complex patients, post-operative patients, older adults, or individuals with high symptom irritability, providers should use clinical judgment and collaborate with the broader medical team when appropriate.
3. Progression Should Be Clear, Small, and Defensible
Progressive overload is central to improving muscular fitness.
But progression does not need to be dramatic.
Estimated safe load increases may include:
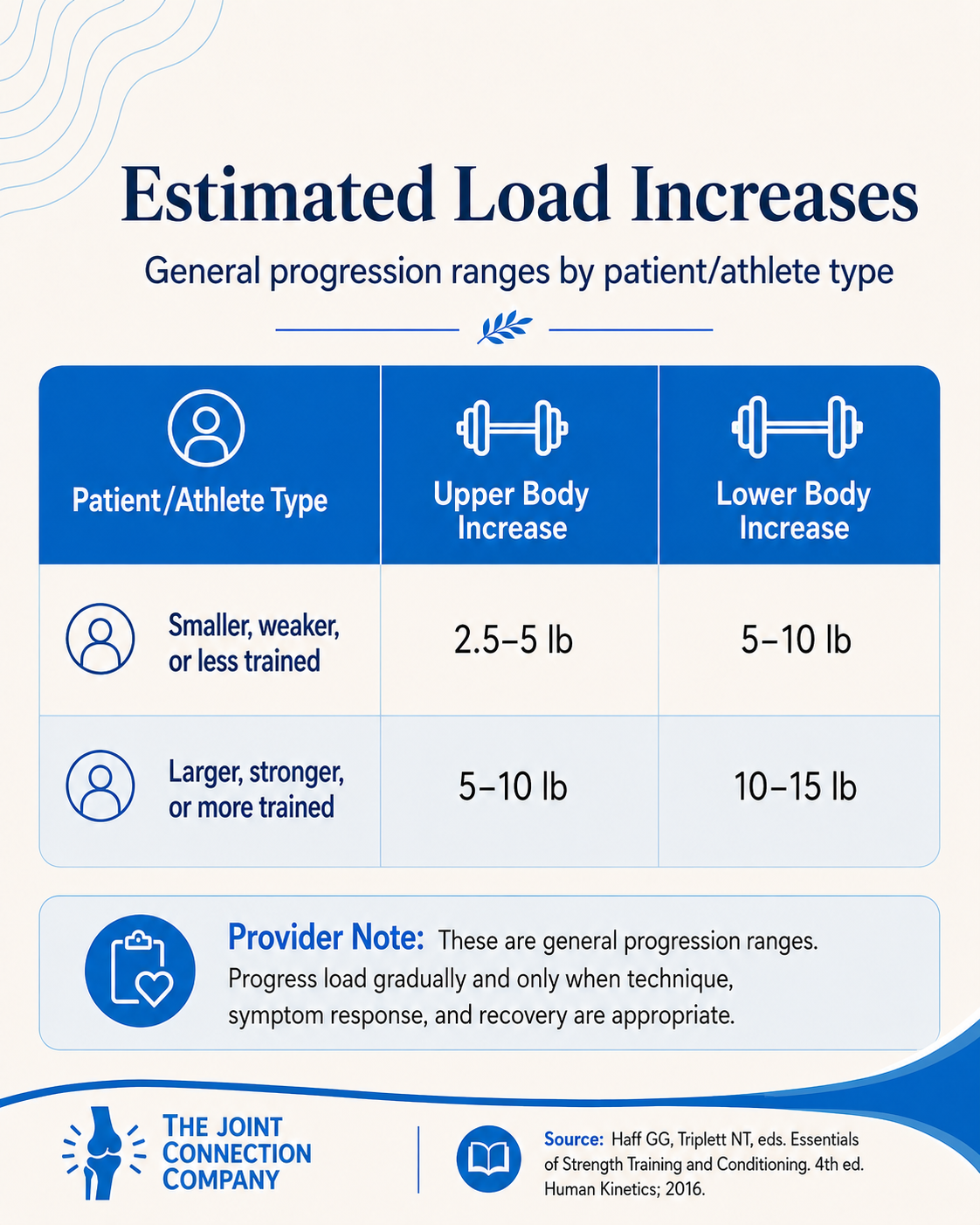
In clinical practice, providers can also progress by modifying:
Sets
Repetitions
Load
Tempo
Rest time
Range of motion
Movement complexity
Exercise order
Frequency
Weekly volume
Environmental challenge
Dual-task demands
A simple progression rule for many patients:
Progress when the patient can complete the current dose with acceptable technique, acceptable symptoms, and acceptable recovery.
That final piece matters.
An exercise that looks fine during the session but causes a major flare for three days may not be the right dose yet.
4. Do Not Overcomplicate the Minimum Effective Dose
For many adults, especially beginners, a reasonable starting point is resistance training at least 2 days per week involving major muscle groups.
From there, providers can adjust based on goals.
For strength, heavier loads tend to matter more.
For hypertrophy, weekly volume becomes more important, with evidence suggesting that higher weekly set volume can support muscle growth.
For endurance, lighter loads and higher repetitions may be more appropriate.
But the provider’s first job is often not optimization. It is initiation.
A patient who is doing nothing does not need the perfect split routine.
They need a starting point.
That might mean:
Two exercises
Two days per week
One set each
A short walking plan
A confidence-based home routine
A supervised gym introduction
A symptom-guided return-to-activity plan
Small starts are not failures.
They are often the first successful exposure.
5. Tie the Prescription to the Patient’s Life
Patients rarely care about “hip abduction strength” in isolation.
They care about:
Stairs
Sleep
Golf
Hiking
Picking up grandchildren
Returning to work
Getting off the floor
Carrying groceries
Running without fear
Traveling without flaring symptoms
Feeling independent again
The exercise prescription should connect to those goals.
Instead of saying:
“We are strengthening your quadriceps.”
Try:
“We are building the strength and control you need to go downstairs with less pain and more confidence.”
Instead of saying:
“We are working on power.”
Try:
“We are training your body to produce force quickly so you can react, step, climb, and move more confidently.”
This is not “dumbing it down.”
This is clinical translation.
6. Use Education to Reduce Fear
Exercise prescription often fails when patients do not understand the difference between hurt, harm, soreness, fatigue, effort, and warning signs.
Providers should clearly explain:
What sensations are expected
What symptoms are acceptable
What symptoms should lead to modification
What symptoms require medical follow-up
How long post-exercise soreness may last
How the patient should respond if symptoms increase
When to contact the provider
This is especially important for patients with chronic pain, persistent symptoms, prior injury, low confidence, or fear of movement.
The goal is not to convince patients to ignore their body.
The goal is to help them interpret their body more accurately.
7. The Real Clinical Skill: From Optimization to Implementation
Clinicians love precision.
We like the best dosage, the best exercise, the best progression, the best protocol.
That matters.
But the most elegant program in the world does not help if the patient does not do it.
The evidence increasingly reminds us that many resistance-training approaches can work when they are appropriately dosed, progressed, and performed consistently.
So perhaps the better clinical mindset is:
Optimize when you can. Simplify when you need to. Individualize always.
Because the true power of exercise prescription is not just in the spreadsheet.
It is in the conversation.
It is in helping someone realize:
“I can move.”
“I can get stronger.”
“I know what to do.”
“I know why it matters.”
“I have a provider who understands me.”
“I am not alone in this process.”
That is where exercise becomes more than a recommendation.
It becomes a relationship-centered intervention.
Clinical Takeaways for Providers
Exercise prescription should be individualized. Start with the person, not the protocol.
Training goals should guide dosage. Strength, power, hypertrophy, and endurance require different loading strategies.
Resistance training does not need to be overly complicated. Consistency, progression, and adherence are often more important than perfect programming.
Mechanotherapy provides a helpful framework. Tissues respond to appropriately dosed mechanical load.
Behavior change is part of the prescription. Education, confidence, shared decision-making, and follow-up are not extras. They are central to success.
Stay within scope. Consider professional, jurisdictional, and personal competence, and collaborate when medical screening or co-management is needed.
📂 Supplemental Information / Citations
Haff GG, Triplett NT, eds. Essentials of Strength Training and Conditioning. 4th ed. Human Kinetics; 2016.
Currier BS, D’Souza AC, Singh MAF, et al. American College of Sports Medicine position stand: resistance training prescription for muscle function, hypertrophy, and physical performance in healthy adults—an overview of reviews. Med Sci Sports Exerc. 2026;58(4):851-872. doi:10.1249/MSS.0000000000003897
Khan KM, Scott A. Mechanotherapy: how physical therapists’ prescription of exercise promotes tissue repair. Br J Sports Med. 2009;43(4):247-252. doi:10.1136/bjsm.2008.054239
Wood L, Ash G. Exercise prescription and patient outcomes. BMC Prim Care. 2025;26(1):233. doi:10.1186/s12875-025-02953-4
Lucini D, Pagani M. Exercise prescription to foster health and well-being: a behavioral approach to transform barriers into opportunities. Int J Environ Res Public Health. 2021;18(3):968. doi:10.3390/ijerph18030968
American Physical Therapy Association. Scope of Practice. Accessed May 25, 2026.
This content drafted, researched, edited, and generated by:
Jackson Kojima, PT, DPT
Jackson Kojima, PT, DPT, OCS is a physical therapist with an extensive background in orthopedics, geriatrics, and sports rehabilitation. Dr. Kojima is a board-certified orthopedic clinical specialist (OCS) with a passion for post-operative rehabilitation and enjoys treating multi-factorial conditions like low back pain and generalized joint pain. Dr. Kojima earned his doctorate of physical therapy from Campbell University in 2021 and currently practices in Greenville, SC.
McKinley Pollock, PT, DPT
McKinley Pollock, PT, DPT, OCS, CSCS is a physical therapist with a background in orthopedics and sports rehabilitation. Dr. Pollock earned his doctorate of physical therapy from Campbell University in 2021, is a board-certified orthopedic clinical specialist (OCS), and certified strength and conditioning specialist (CSCS). Dr. Pollock enjoys combining lessons learned from his DPT training and research, translating these into clinical practice. His passions include promoting relationships between patients & clinicians to promote clinical effectiveness, satisfaction, and efficiency, the implementation of primary preventative medicine into clinical practice, and leadership and education development.
© 2026 The Joint Connection Company. All rights reserved.
The content on this website, including all text, graphics, and materials, is the exclusive property of The Joint Connection Company and is protected by applicable copyright and intellectual property laws. No part of this site may be reproduced, distributed, or used without prior written permission.