

❤️ POTS, Dizziness, and a Racing Heart: Why the Conversation Matters
Blog title image for “POTS, Dizziness, and a Racing Heart: Why the Conversation Matters.” The graphic shows two illustrated healthcare providers in a warm, welcoming physical therapy setting. One provider in a teal shirt is seated on a recumbent bike, smiling while exercising. A second provider in a light gray polo stands beside him holding a clipboard and gesturing supportively, suggesting coaching, education, and conversation. Behind them are teal icons representing dizziness and heart rate, including a swirl symbol and an ECG heartbeat line. The left side of the image features the blog title in large dark teal text, with The Joint Connection Company branding at the bottom. The overall style is clean, professional, friendly, and uses a teal-and-cream color palette.
✨ Too Long Didn’t Read (TL;DR) / Summary
Postural Orthostatic Tachycardia Syndrome, better known as POTS, is a condition involving symptoms of orthostatic intolerance. That means symptoms tend to show up or worsen when someone moves into an upright position, such as sitting or standing, and often improve when lying down.
Commonly reported symptoms can include lightheadedness, dizziness, palpitations, racing heart, fatigue, exercise intolerance, nausea, headache, “brain fog,” weakness, and feeling worse in heat or after prolonged standing.
Symptoms alone do not diagnose POTS.
Many conditions can look similar, including dehydration, anemia, thyroid disease, medication effects, cardiac rhythm problems, orthostatic hypotension, vasovagal syncope, infection, anxiety, deconditioning, and other medical concerns.
For patients, this means:
You are not “making it up,” and you also deserve a careful evaluation.
For providers, this means:
We should validate symptoms, screen thoughtfully, recognize when referral is needed, and help patients build safe, progressive strategies to improve function.
🧾 Condition-Specific General Information
What is POTS?
POTS stands for Postural Orthostatic Tachycardia Syndrome.
The name gives us a few clues:
Postural = related to body position
Orthostatic = related to being upright
Tachycardia = increased heart rate
Syndrome = a collection of signs and symptoms, not one single disease process
POTS is generally described as a form of orthostatic intolerance, where symptoms occur or worsen in the upright position and are associated with an excessive increase in heart rate without a significant drop in blood pressure.
In many clinical descriptions, POTS involves a heart rate increase of at least 30 beats per minute in adults, or at least 40 beats per minute in adolescents, within about 10 minutes of standing or head-up tilt, without orthostatic hypotension.
That sounds simple on paper.
In real life, it is often much more complicated.
Heart rate can change for a number of reasons: hydration, heat, medications, illness, stress, sleep, caffeine, pain, anxiety, deconditioning, blood volume, and more.
This is one reason experts emphasize that POTS should not be diagnosed from one symptom, one smartwatch reading, or one bad day.
Why POTS can be confusing
POTS is not just “feeling dizzy.”
It is also not just “having a high heart rate.”
And it is definitely not just “being anxious.”
POTS can involve symptoms across several body systems, including cardiovascular, neurologic, gastrointestinal, musculoskeletal, and general fatigue-related complaints. But many of those symptoms are also nonspecific, meaning they can happen in many other conditions.
Common symptoms may include:
Dizziness or lightheadedness
Palpitations or racing heart
Feeling faint or near-fainting
Exercise intolerance
Fatigue
Weakness
Brain fog
Headache or migraine
Nausea, bloating, diarrhea, or abdominal discomfort
Heat intolerance
Shakiness or tremulousness
Shortness of breath or chest discomfort
Sleep disturbance
Muscle fatigue or pain
This is why a careful clinical conversation matters.
A patient might say:
“Every time I stand up, my heart races and I feel like I am going to pass out.”
That should not be dismissed.
But it also should not automatically be labeled POTS without asking more questions, checking vital signs, reviewing medications, and considering whether another condition may be contributing.
Symptoms alone are not enough
One of the major themes in the POTS literature is that symptoms alone cannot confirm the diagnosis.
That matters because many treatable medical conditions can mimic POTS-like symptoms. These may include:
Dehydration or low blood volume
Medication side effects
Anemia (low red blood cell counts)
Thyroid disease
Infection or recent illness
Orthostatic hypotension
Vasovagal syncope
Inappropriate sinus tachycardia
Cardiac rhythm abnormalities
Deconditioning after illness, bedrest, surgery, or prolonged inactivity
Migraine, vestibular disorders, or neurologic conditions
Autoimmune or inflammatory conditions
Connective tissue disorders or hypermobility-related concerns
Gastrointestinal disorders
Pelvic pain or bladder-related conditions
This does not mean a patient’s symptoms are “not real.”
It means the symptoms deserve a thoughtful workup.
A good healthcare interaction should sound less like:
“It is probably just anxiety.”
And more like:
“Your symptoms are real. Let’s look at the pattern, your vital signs, your medical history, your activity tolerance, and whether anything else needs to be ruled out.”
That difference matters.
The role of position: a key clinical clue
A major feature of POTS is that symptoms are typically tied to upright posture.
That means providers often want to know:
Do symptoms worsen when standing?
Do symptoms improve when lying down?
How long does it take for symptoms to appear?
Are symptoms worse in the morning?
Are symptoms worse after heat exposure, prolonged standing, dehydration, illness, or large meals?
Does the heart rate rise in a reproducible way when moving from lying down to standing?
Is blood pressure dropping during certain positions?
Are there symptoms that do not seem related to posture?
That last question is important.
If someone has fatigue, brain fog, nausea, headache, or pain all day regardless of position, those symptoms still matter, but they may not be fully explained by POTS alone. They may require additional evaluation and a broader treatment plan.
What is an active stand test?
An active stand test is one way clinicians may screen for several different orthostatic changes.
In a typical version, the patient lies quietly for several minutes while resting heart rate and blood pressure are measured. Then the patient stands, and heart rate and blood pressure are monitored at intervals, often at 1, 3, 5, and 10 minutes.
This can help clinicians observe whether symptoms line up with changes in heart rate and blood pressure.
However, this is not something patients should use to self-diagnose without clinical guidance. Testing conditions matter. Hydration, time of day, medications, anxiety, recent meals, caffeine, illness, and measurement accuracy can all influence results.
The active stand test is best viewed as one piece of the puzzle, not the whole picture.
Where exercise fits in
Here is where physical therapy, occupational therapy, and personal traininig becomes especially relevant.
Many people with POTS or POTS-like orthostatic intolerance struggle with exercise intolerance. They may want to be active but feel worse when they try. This can create a frustrating cycle:
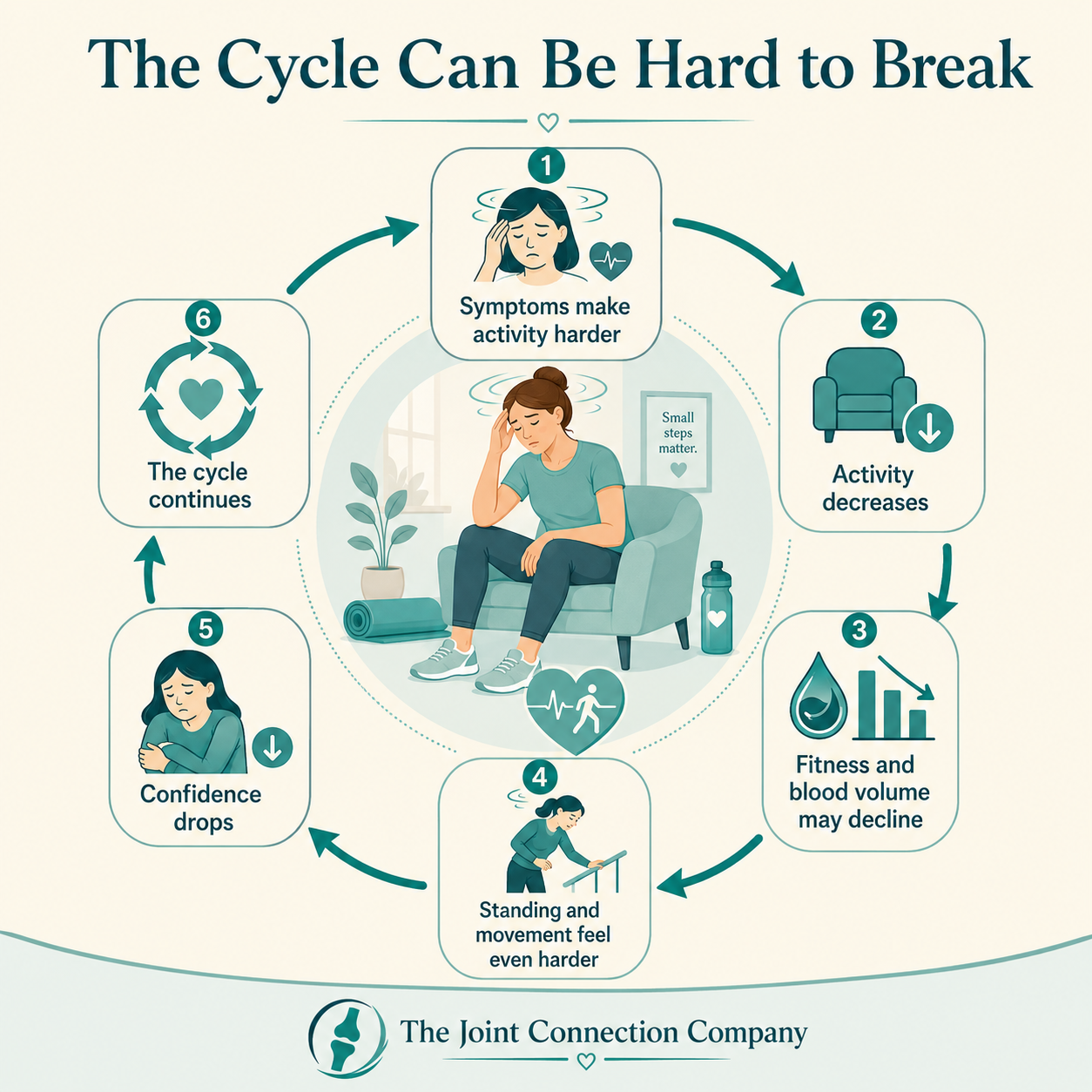
Infographic titled “The Cycle Can Be Hard to Break” showing a circular six-step cycle related to POTS symptoms and reduced activity. In the center, a tired-looking woman sits slumped in a chair with one hand on her forehead, surrounded by subtle dizziness lines. Around her are six connected boxes with arrows moving clockwise. Step 1 says “Symptoms make activity harder” and shows a person feeling dizzy. Step 2 says “Activity decreases” with a chair icon. Step 3 says “Fitness and blood volume may decline” with a droplet and downward graph. Step 4 says “Standing and movement feel even harder” with a person leaning on a railing. Step 5 says “Confidence drops” with a sad figure. Step 6 says “The cycle continues” with circular arrows around a heart. The graphic uses a calm teal-and-cream color palette and includes The Joint Connection Company branding at the bottom.
Research has shown that structured, progressive exercise training can be helpful for many people with POTS, especially when it starts in positions that reduce orthostatic stress, such as rowing, swimming, or recumbent biking.
This is not the same as telling someone to “just exercise.”
There are literally hundreds of ways to “just exercise.” That phrase is usually not helpful.
A better message is:
“Your body may need a more strategic entry point. We may need to begin with positions and intensities your system can tolerate, then gradually build capacity.”
Early exercise programming for POTS often emphasizes:
Recumbent or semi-recumbent cardiovascular exercise
Gradual progression of duration and intensity
Resistance training to improve skeletal muscle strength
Lower body and trunk strengthening
Careful monitoring of symptoms, heart rate, blood pressure, and recovery
Education on pacing, hydration, heat, and symptom triggers
Progressing toward upright exercise when tolerated
Exercise is not a magic switch, and not every symptom improves immediately. Some patients may initially feel more fatigued when starting a program. That does not mean the plan has failed. It may mean the plan needs to be adjusted, slowed down, supervised more closely, or coordinated with the broader medical team.
Practical strategies patients may discuss with their healthcare team
Depending on the individual person and medical history, healthcare teams may discuss non-pharmacologic strategies such as:
Hydration strategies
Salt intake guidance when medically appropriate
Compression garments
Avoiding prolonged standing
Avoiding excessive heat exposure
Smaller, more frequent meals if symptoms worsen after eating
Gradual physical reconditioning
Recumbent or semi-recumbent exercise
Resistance training
Physical counter-maneuvers, such as leg crossing, muscle tensing, or squatting when symptoms begin
Sleep, stress, and recovery routines
Referral to cardiology, neurology, primary care, vestibular specialists, gastroenterology, behavioral health, or other providers when appropriate
Important note: hydration, sodium, compression, and medication decisions should be individualized. Patients with blood pressure concerns, kidney disease, cardiac conditions, pregnancy, eating disorders, medication interactions, or other medical considerations should not make major changes without medical guidance.
What patients should ask their provider
If you suspect POTS or orthostatic intolerance, consider asking:
“Could my symptoms be related to changes in heart rate or blood pressure when I stand?”
“Should we check orthostatic vital signs or consider an active stand test?”
“Are there conditions we should rule out, such as anemia, thyroid issues, medication effects, dehydration, cardiac rhythm problems, or orthostatic hypotension?”
“Do my symptoms improve when lying down, or are they present regardless of position?”
“Would a referral to cardiology, neurology, or another specialist be appropriate?”
“Would physical therapy or supervised exercise help me safely rebuild activity tolerance?”
“What symptoms would be considered red flags?”
When to seek urgent medical care
Seek urgent or emergency medical care if symptoms include:
Chest pain that is severe, new, or concerning
Fainting with injury
New shortness of breath at rest
New neurologic symptoms, such as facial droop, one-sided weakness, severe sudden headache, or difficulty speaking
Heart rhythm symptoms that feel sudden, irregular, or severe
Symptoms after possible dehydration, infection, blood loss, or medication reaction
Severe worsening or symptoms that feel unsafe
When in doubt, it is better to be checked.
👩⚕️ For Providers 👨⚕️
Start with validation, then investigate
Patients with suspected POTS often arrive after months or years of being told their symptoms are “just stress,” “just anxiety,” or “just being out of shape.”
That history can shape the whole encounter.
The first therapeutic intervention may be how we respond.
A strong opening sounds like:
“I believe that what you are feeling is real. Our job is to understand what is driving it and who needs to be involved in your care.”
That statement does two important things at once: it validates the patient and preserves clinical reasoning.
Avoid two common errors
When working with patients who present with dizziness, tachycardia, fatigue, and exercise intolerance, providers can fall into two opposite traps.
Trap #1: Dismissing the symptoms.
This can damage trust and delay care.
Trap #2: Over-labeling symptoms as POTS without sufficient evidence.
This can also be harmful because other treatable conditions may be missed.
The more nuanced approach is to say:
“POTS is one possibility, but orthostatic symptoms and tachycardia can happen for many reasons. Let’s gather better information.”
Keep in mind to stay within the scope of your professional practice and license. Even if you suspect a certain diagnosis, ensure that you follow your individual scope.
Screening considerations
Within the scope of PT practice, physical therapists may contribute through careful history-taking, systems review, vital sign monitoring, functional testing, exercise assessment, and referral when findings are outside the expected presentation or outside the PT’s scope.
This aligns with the broader role of physical therapists in helping people improve movement, function, chronic disease management, prevention, and health-related goals, while practicing within applicable state rules and jurisdictional scope.
Relevant clinical questions may include:
Are symptoms clearly worse upright?
Do symptoms improve when supine?
Are symptoms reproducible?
How long have symptoms been present?
Is there a recent trigger, such as illness, surgery, concussion, pregnancy, prolonged bedrest, or major activity reduction?
Are there medication changes or substances that could influence heart rate or blood pressure?
Are there signs of orthostatic hypotension?
Is the rhythm regular or irregular?
Are symptoms disproportionate, progressive, or associated with red flags?
Are there comorbid conditions that need co-management?
Has the patient already been medically evaluated?
Active stand testing: helpful, but not casual
The active stand test can be clinically useful, but it should be performed thoughtfully. Bryarly and colleagues describe a process involving supine rest followed by monitoring heart rate and blood pressure during standing, commonly at intervals through 10 minutes.
The key is not to use this as a standalone diagnostic tool. Instead, it can help determine whether the patient’s symptoms and vital sign responses warrant medical referral, additional communication with the care team, or modification of the exercise plan.
Documentation may include:
Resting position and duration
Baseline HR and BP
Standing HR and BP at defined intervals
Symptoms at each interval
Whether symptoms resolved when sitting or lying down
Relevant contextual factors: hydration, time of day, medication timing, heat exposure, recent meals, caffeine, sleep, illness
Clinical response and referral decision-making
Red flags and referral considerations
Referral or medical co-management should be considered when symptoms include:
Syncope or recurrent near-syncope
Chest pain
New or worsening shortness of breath
Irregular rhythm
Significant blood pressure drop
New neurologic symptoms
Unexplained weight loss
Fever, systemic illness, or signs of infection
Suspected anemia, thyroid dysfunction, cardiac pathology, pulmonary pathology, or medication-related tachycardia
Symptoms not clearly linked to posture
Symptoms outside the treating provider’s training, setting, or scope
POTS-like symptoms can overlap with multiple medical conditions. Olshansky and colleagues strongly emphasize that symptoms alone are insufficient and that serious or treatable underlying causes may be missed when the label “POTS” is applied too loosely.
Exercise programming: make it strategic
Exercise is one of the most important areas where PTs can contribute.
But the dosage matters.
A patient with orthostatic intolerance may not tolerate a traditional upright conditioning program at first. Exercise programming often needs to begin with lower orthostatic load options, such as:
Recumbent bike
Rowing
Swimming
Supine or seated strengthening
Floor-based trunk and hip strengthening
Gradual lower extremity resistance training
Carefully dosed intervals
Longer rest breaks
Symptom-guided progression
Fu and Levine describe horizontal exercise early in care as a key strategy because it allows conditioning while reducing the upright posture that often provokes symptoms. Bryarly and colleagues also emphasize progressive exercise training and resistance training as important parts of management for many patients.
Suggested PT progression framework
This is not a protocol for every patient. It is a clinical reasoning framework. Dosing and consideration must be individualized.
Phase 1: Calm the entry point
Goal: Find tolerable movement.
Examples: diaphragmatic breathing, gentle mobility, recumbent cycling, low-load mat strengthening, symptom education, hydration discussion within medical guidance, and activity pacing.
Phase 2: Build the base
Goal: Improve consistency.
Examples: recumbent cardio intervals, rowing, swimming, progressive resistance training, lower extremity strengthening, trunk strengthening, and recovery monitoring.
Phase 3: Add upright tolerance
Goal: Gradually expose the patient to more upright activity.
Examples: seated-to-standing exercise transitions, short bouts of standing strength work, walking intervals, step-ups, carries, and functional conditioning.
Phase 4: Reconnect with life
Goal: Return to school, work, exercise, recreation, parenting, athletics, and meaningful activities.
Examples: sport-specific or job-specific conditioning, community walking, gym programming, independent self-management, and long-term wellness planning.
Communication matters as much as the exercise
Patients with POTS-like symptoms often feel betrayed by their body.
They may be afraid to stand.
Afraid to exercise.
Afraid to shower.
Afraid to go to class.
Afraid to go to work.
Afraid to be dismissed again.
So the provider’s language matters.
Instead of:
“You’re just deconditioned.”
Try:
“Your system may be having trouble tolerating upright stress right now. We can work on rebuilding that tolerance gradually.”
Instead of:
“You need to push harder.”
Try:
“We need the right challenge at the right dose so your body can adapt without constantly crashing.”
Instead of:
“Your tests are normal.”
Try:
“It is good that we are not seeing certain dangerous findings. Now let’s keep working to understand why you still feel this way.”
The relationship is not extra.
The relationship is part of the intervention.
What providers should avoid
Providers should avoid:
Diagnosing POTS solely from symptoms
Treating unexplained tachycardia without appropriate screening
Ignoring blood pressure responses
Assuming anxiety is the cause
Assuming POTS explains every symptom
Overprescribing upright exercise too early
Telling patients to simply “push through”
Providing medication advice outside scope
Recommending major sodium or fluid changes without considering medical history
Missing referral signs
Conclusion and Reflection:
POTS care is not just about heart rate.
It is about pattern recognition, safety, education, communication, graded exposure, strength, cardiovascular conditioning, and team-based care.
Patients need providers who are curious enough to investigate and compassionate enough to stay connected.
Providers need to balance validation with clinical precision.
That is where better conversations create better care.
Key Takeaways
POTS is generally characterized by orthostatic symptoms with excessive heart rate increase during upright posture, without orthostatic hypotension.
Symptoms alone are not enough to diagnose POTS.
Many medical conditions can mimic POTS-like symptoms and should be considered during evaluation.
Active stand testing can help evaluate orthostatic heart rate and blood pressure responses, but it should be interpreted in clinical context.
Exercise training, especially beginning with recumbent or horizontal exercise and progressing gradually, is one of the best-supported nonpharmacologic strategies for many patients with POTS.
Physical therapists can play an important role in screening, monitoring, education, exercise prescription, functional progression, and referral/collaboration when appropriate.
📂 Supplemental Information / Citations
Olshansky B, Cannom D, Fedorowski A, et al. Postural Orthostatic Tachycardia Syndrome (POTS): a critical assessment. Prog Cardiovasc Dis. 2020;63(3):263-270. doi:10.1016/j.pcad.2020.03.010
Bryarly M, Phillips LT, Fu Q, Vernino S, Levine BD. Postural Orthostatic Tachycardia Syndrome: JACC Focus Seminar. J Am Coll Cardiol. 2019;73(10):1207-1228. doi:10.1016/j.jacc.2018.11.059
Fu Q, Levine BD. Exercise and non-pharmacological treatment of POTS. Auton Neurosci. 2018;215:20-27. doi:10.1016/j.autneu.2018.07.001
Sheldon RS, Grubb BP II, Olshansky B, et al. 2015 Heart Rhythm Society Expert Consensus Statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm.2015;12(6):e41-e63. doi:10.1016/j.hrthm.2015.03.029
Trimble KZ, Switzer JN, Blitshteyn S. Exercise in Postural Orthostatic Tachycardia Syndrome: Focus on Individualized Exercise Approach. J Clin Med. 2024 Nov 9;13(22):6747. doi: 10.3390/jcm13226747. PMID: 39597891; PMCID: PMC11594886.
Ghazal M, Akkawi AR, Fancher A, Oundo E, Tanzeem H, Sajjad L, Briasoulis A. Pathophysiology and management of postural orthostatic tachycardia syndrome (POTS): A literature review. Curr Probl Cardiol. 2025 Mar;50(3):102977. doi: 10.1016/j.cpcardiol.2024.102977. Epub 2024 Dec 18. PMID: 39706392.
American Physical Therapy Association. Find a PT. ChoosePT. Accessed May 20, 2026. https://www.choosept.com/find-a-pt
North Carolina Board of Physical Therapy Examiners. Scope of Practice. Accessed May 20, 2026. https://www2.ncptboard.org/app/LandingPages/ScopeOfPracticeHome.php
This content drafted, researched, edited, and generated by:
McKinley Pollock, PT, DPT
McKinley Pollock, PT, DPT, OCS, CSCS is a physical therapist with a background in orthopedics and sports rehabilitation. Dr. Pollock earned his doctorate of physical therapy from Campbell University in 2021, is a board-certified orthopedic clinical specialist (OCS), and certified strength and conditioning specialist (CSCS). Dr. Pollock enjoys combining lessons learned from his DPT training and research, translating these into clinical practice. His passions include promoting relationships between patients & clinicians to promote clinical effectiveness, satisfaction, and efficiency, the implementation of primary preventative medicine into clinical practice, and leadership and education development.
© 2026 The Joint Connection Company. All rights reserved.
The content on this website, including all text, graphics, and materials, is the exclusive property of The Joint Connection Company and is protected by applicable copyright and intellectual property laws. No part of this site may be reproduced, distributed, or used without prior written permission.